Introduction:
Interocclusal registration materials record the occlusal relationship between natural and/or artificial teeth for planning occlusal rehabilitation and for construction of removable and fixed partial dentures. According to Dawson[6], criteria for accuracy in making interocclusal records include the following points (1) the recording material must not cause any movement of teeth or displacement of soft tissues, (2) the recording material must fit casts as accurately as the teeth intraorally (3) the accuracy of the jaw relation record should check in the mouth and on the casts. The cause of occlusal discrepancies attributable to the interocclusal record can be divided into three categories one cause is related to the biologic characteristics of the somatognathic system, and a second cause is attributed to iatrogenic errors related to manipulation of the material[9]. The third cause is associated with the properties of the interocclusal recording material and an inappropriate relationship of the maxillary to the mandibular casts on an articulator[2],[7],[11],[12],[13],[14],[15],[16]. An inaccurate transfer of the interocclusal records results in poor mounting of the casts in the articulator with concomitant diagnostic and treatment errors[2].During the process of transferring the relations, changes are common in the vertical and horizontal dimensions of the position of the jaws. A material inserted between the maxillary and mandibular teeth can cause deviation from a normal intercuspal position in the vertical, anteroposterior, mediolateral and combined directions[1]. Ideally the material used to obtain precise interocclusal records should offer no resistance to closure, have desired flow and permit the masticatory mechanism to operate free from any interference. Plaster, modeling compound, wax, and acrylic resin are materials routinely used for the registration of the occlusal relationship. Some are difficult to use; that is, they are brittle, unstable, and/or inaccurate[3]. Zinc oxide pastes and elastomers are the most popular materials for making interocclusal records[2],[16] polyvinyl siloxane material for inter dental records was reported to have high dimensional accuracy and ease of manipulation[5]. In the present study, an attempt has been made to evaluate and compare the clinical accuracy of three interocclusal recording materials and to find out the most accurate material that can be used in routine clinical practice.
Materials And Methods:
The subjects for this study were selected from the department of Prosthodontics. Ten subjects of both the sexes were included in the study. Subjects were in the age group of 21 to 30 years. The criteria for selection were that the subjects possessed a full complement of teeth (excluding third molars); there was no history of TMJ dysfunction or MPD syndrome, no carious, hypoplastic or broken teeth, with sparse restorative treatment and adequate posterior and anterior occlusal stops. The following materials and equipments were used in this study: Rim-Lock impression trays-used for irreversible hydrocolloid impressions of the subjects. Bite registration trays[1]-used for carrying interocclusal registration materials. Irreversible hydrocolloid impression material[1] was used for impressions of each arch of the subjects studied. All casts were poured in, Dental stone[2] plaster Class-Ill. A Whip-mix articulator (Semi adjustable arcon type) and a whip-mix arbitrary face bow were used in this study. Three types of interocclusal registration materials were used. Pink modelling wax sheets, Zinc OxideEugenol Bite Registration Paste and Vinyl Polysiloxane Bite registration Material were used for interocclusal records. Graph paper with 1 mm squares reinforced with card-sheet was also used. The reinforcement reduced distortion on the graph paper while the recordings were being made. Inks of different colours were used to designate individual recording. Red ink was used to record position of hand articulated casts on graph paper. Black ink was used to record position of casts with wax interocclusal records. Blue ink was used to record position of casts with vinyl polysiloxane interocclusal records. Green ink was used to record position of casts with zinc oxide eugenol interocclusal records.
Method:
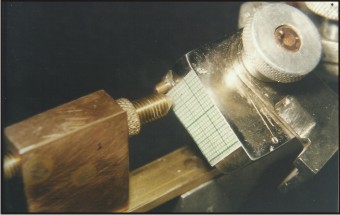
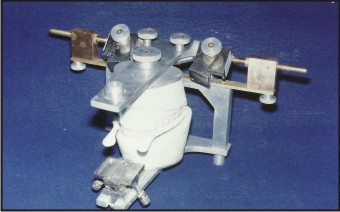
Irreversible hydrocolloid impressions of each arch were taken for each patient. These were immediately poured in stone and mounted on a Whip-Mix articulator with the arbitrary face-bow. With hand articulation the mandibular cast was mounted to the maxillary cast in maximum intercuspation. The interocclusal record with each material was taken three times, for each subject i.e. for each subject three wax interocclusal records, three Zinc oxide eugenol records and three Vinyl Polysiloxane records were made.The condylar spheres were removed from the articulator and replaced by the attachment of a Buhnergraph (Fig. 1). Maxillary casts of each patient were mounted with an arbitrary face-bow on an arcon articulator and the mandibular casts were carefully hand-mounted to the upper casts in maximum intercuspal position (Fig. 2). Graph paper with 1 mm squares was attached to card sheet for reinforcement and placed on the outer surface of the condylar housing of the articulator (Fig. 3). Red ink was placed on the Buhnergraph styli. The position of the tips of the inked styli was marked on the graph paper. This point was designated as point O. The styli were then removed and cleaned, and a different colour of ink was placed on them. An interocclusal record was placed on the maxillary cast, the mandibular cast was set in the record and both casts were carefully supported in the imprints of the record (Fig. 4). Again the positions of the tips of the styli were marked on the graph paper and the point obtained was designated as point R. The procedure was repeated for each interocclusal record. Measurements of the right and left condyle were recorded for each interocclusal record. In order to obtain precise results, the graph paper obtained after recording from samples were scanned and the size of image was increased proportionately. The enlarged images were then exported to CorelDraw for further measurement of the distance between two points i.e. point O and point R. (Fig. 5). The centers of the points were assumed as the centers around which the density of the pixels was highest. Now two perpendiculars were dropped each from the center of each point. The point where they crossed each other was taken as base point for measurement. The vertical distance from this base point to the center of one point was taken as distance in Y-axis direction (vertical displacement) while the horizontal distance from this point to the center of the other point was measured as distance in X-axis direction (anteroposterior displacement). The values were measured upto three decimal points (Fig. 6). Deviations measured (distance from Point O to Point R in mm) with different interocclusal records were divided into three groups:
 | Fig 1 : Showing Buhnergraph Attached To Whip-mix Articulator
 |
 | Fig 2 : Showing Maxillary And Mandibular Casts In Maximum Intercuspal Position
|
 | Fig 3 : Showing Inked Styli, Recording Position Of Casts On Graph Paper
|
 | Fig 4 : Showing Maxillary And Mandibular Cast With Interocclusal Record
|
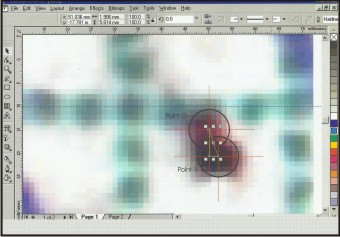 | Fig 5 : Showing Distance Between Two Points
|
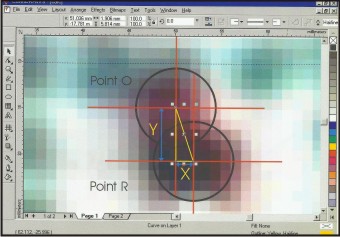 | Fig 6 : Showing Distance Between Two Points On Y-axis And X-axis
|
Group A: Deviation measured with Wax interocclusal records
Group B: Deviation measured with Zinc oxide eugenol interocclusal records
Group C: Deviation measured with Vinyl polysiloxane interocclusal records
Each group was further divided in two subgroups as for each subject deviation on right and left side was measured separately.
Group A- (1) GroupAR (2) GroupAL
Group B- (1) GroupBR (2) GroupBL
Group C- (1) GroupCR (2) GroupCL
Statistical analysis of the available data was carried out to ascertain the level of significance of various observations.
Discussion:
Recording maxillomandibular relationship is an important step in oral rehabilitation. There are various methods of recording maxillomandibular relationships[18]. Direct interocclusal record is the most commonly used method because of its simplicity. Ten subjects with full complement of teeth and sparse restorative treatment were selected for this study. This was done to reduce the probability of any occlusal prematurity. As the proprioceptors in the periodontal ligaments of the prematurely contacting teeth will reflexly guide the mandible into the undesired centric occlusion position[23]. It was also considered that the subjects did not have any history of TMJ dysfunction as in mandibular dysfunction patients, the mandible may not assume a stable comfortable position before making a centric jaw registration[8],[10],[22]. Because materials for recording interocclusal relationships are used to transfer the position of the jaws to an articulator, the choice of material is important. Wax was used as an interocclusal recording material in the present study because it is one of the oldest and most useful materials in dentistry, its thermoplastic properties make its application simple. When waxes are compared with other available recording medium, they are decidedly inferior. However, waxes are still the most popular material because of cost and ease of manipulation[1]. Zinc oxide eugenol bite registration paste was used because it is a reliable interocclusal recording material. It shows low resistance to closure (0.5 to 0.6 N) than silicones, polyether and acrylic resin materials. The volumetric changes during registration and up to 30 minutes of storage were less than 0.5%[12]. Addition type silicones were introduced as an accurate and dimensionally stable interocclusal recording material[5]. The vinyl polysiloxane interocclusal registering material was used in the study with the help of auto mixing system. The material comes as a twin barreled syringe, each side of which extrudes an equal volume of material simultaneously through a disposable mixing tip, when loaded on a dispensing gun. The auto mixing concept is an improvement over the traditional method of mixing two pastes by hand spatulation. Uniform ratios of catalyst and base are always dispensed, which results in consistent mixing every time.
After selection of material, interocclusal record of each subject was taken three times with each material. This was done to minimize the iatrogenic errors i.e. related to manipulation of materials and errors related to the subjects i.e. deviation from the centric occlusion position after placing the interocclusal recording material[9].
The maxillary casts of all subjects selected for the study were mounted on a whip mix articulator with the help of arbitrary facebow. This facebow transfer allowed a more accurate arc of closure on the articulator when the interocclusal records are removed and the articulator is closed[4]. After mounting the maxillary cast on the whip-mix articulator with the help of facebow, the mandibular cast was mounted in maximum intercuspation ensuring adequate anterior and posterior occlusal stops in position thereby eliminating any possibility of instability[19],[20],[21].
The accuracy of recording material was evaluated by measuring the displacement of articulator hinge axis from its original position (the position without interocclusal record). To record thisdisplacement, a Buhnergraph was used in the present study. A Buhnergraph can record the vertical and anteroposterior displacement of articulator hinge axis while the other methods can record only the vertical change induced by the interocclusal recording material[1],[15].
Group A (wax interocclusal records) showed highest mean vertical deviation (1.3492 mm) and highest mean anteroposterior deviation (0.2956 mm) on both right and left side of subjects (Table 1). The higher deviation observed with group A could be because of its greater resistance to closure, low dimensional stability and distortion on removal[11]. The dimensional stability of wax is also difficult to maintain because of its high thermal coefficient. Wax had the highest coefficient of thermal expansion (350 x 10-6/OC). Many studies[13],[14],[15],[17] were conducted on wax regarding its properties as an interocclusal recording material confirmed the present results.
Group B (Zinc oxide eugenol interocclusal records) occupied an intermediate position between group A and group C for mean vertical deviation (0.7384 mm) and mean anteroposterior deviation (0.2328 mm) on both right and left side of subjects (Table-1). Despite its good physical properties considerable deviation was observed with zinc oxide eugenol interocclusal records. Some of the factors responsible for the observed deviation could be: - (1) it, cracks and sticks to the teeth on removal from the mouth. Therefore the vital portions of record were lost through breakage; (2) the flash around the teeth prevented the accurate seating of casts. It is advisable to use a minimum amount of zinc oxide eugenol to avoid excess flash; (3) Interference from the carrier was also one of the factors responsible for the observed deviations. Carrier interferes with centric jaw closure by touching the inner surface of cheeks, tongue and other soft tissues[7].
Group C (Vinyl Polysiloxane interocclusal record) exhibited least mean deviation in the vertical and anteroposterior direction (Table-1). Although polyvinyl siloxane interocciusal recording material showed least deviation (0.1892 mm in vertical direction and 0.0524 mm in anteroposterior direction), it has certain shortcomings, which may be responsible for the deviations observed. Polyvinyl siloxane material has a brief working time. An increase in viscosity coupled with the development of elasticity could cause distortion in interocclusal registration[12]. Polyvinyl siloxane material showed low initial resistance to closure but a rapid rise of resistance was seen during the working time[11].
Conclusion:
The present study was a clinical study therefore; certain factors could not be controlled although they had a pronounced effect on the accuracy of the recording materials. These factors are (1) temperature; (2) humidity; (3) closing pressure of the patient.
From the observation and analysis done in the study following conclusions had been drawn:
1. Vinyl polysiloxane was the most accurate interocclusal recording material. The deviation with vinyl polysiloxane was found statistically non-significant.
2. Zinc oxide eugenol bite registration paste was the next most accurate recording material. The deviation observed was 0.7384 mm to 0.5818 mm in vertical direction and 0.2328 mm to 0.2042 mm in anteroposterior direction.
3. Wax was found consistently unreliable interocclusal recording material. The deviation observed was 1.0340 to 1.3492 mm. in vertical direction and 0.2024 to 0.2956 in anteroposterior direction.
4. The deviation was found more in a vertical direction, followed by an anteroposterior direction for all the materials.
5. No significant difference was found in vertical and anteroposterior deviation when compared for right and left side of subjects.
References:
1. Assif D, Himel R, Grajower Y. A new electromechanical device to measure the accuracy of interocclusal records. J. Prosthet Dent. 1 988; 59(6):672-76.
2. Balthazar-Hart Y, Sandrik JL, Malone WFP, Mazur B, Ha T. Accuracy and dimensional stability of four interocclusal recording materials. 1981; 45(6):586-91.
3. Berman MH. Accurate interocclusal records, J. Prosthet Dent. 1960; 10:620.
4. Boucher’s Prosthodontic Treatment for edentulous patient ed 10, the C. V. Mosby Co. 1990:248.
5. Breeding LC, Dixon DL, Kinderknecht KE. Accuracy of three interocclusal recording materials used to mount a working cast. J. Prosthet. Dent. 1994; 71:265-270.
6. Dawson PE. Evaluation, diagnosis and treatment of occlusal problems. St Louis Mosby 1989; 47:55.
7. Fattore LD, Malone WF, Sandrik JL, Mazur B, Hart T. Clinical evaluation of the accuracy of interocclusal recording materials. J. Prosthet Dent. 1984; 51 (2):153-7.
8. Huffman RW, Regenos JW, Taylor KR. Principles of occlusion, ed. Columbus Ohio. 1980.
9. Kapur KK, Yurkstas AA An evaluation of centric relation records obtained by various techniques J. Prosthet Dent. 1957; 7:770-86.
10. Kornfield M. Mouth Rehabilitation, clinical and laboratory procedures, ed 2 St lous, 1974.
11. Lassila V. Comparison of five interocclusal recording materials. J. Prosthet Dent. 1986; 55:21 5-8.
12. Lassila V, McCabe JF. Properties of interocclusal registration material. J. Prosthet Dent. 1 985; 53:100-4.
13. Millstein PL, Clark RE, Kronmon JH. Determination of the accuracy of wax interocclusal registrations. J. Prosthet Dent. 1971; 25:189.
14. Millstein PL, Clark RE, Kronmon JH Determination of the accuracy of wax interocclusal registrations Part-IL J. Prosthet Dent. 1973; 29:40.
15. Millstein PL, Clark RE. Determination of the accuracy of laminated wax interocclusal wafers. J. Prosthet Dent. 1983; 50(3):327-31.
16. Millstein PL, Hsu CC. Differential accuracy of elastomeric recording materials and associated weight change. J. Prosthet Dent. 1994; 71:400-3.
17. Muller Gotz G Horz W, Kraft E. An experimental study on the influence of the derived casts of the accuracy of different recording materials. Part-Il : Polyether, acrylic resin and corrected wax wafer. J. Prosthet Dent. 1990; 63(4):389-95.
18. Myers ML. Centric relation records-historical review. J. Prosthet Dent. 1982; 47(2):141-45.
19. Strohaver RA. A comparison of articulator mountings made with centric relation and myocentric position records J. Prosthet Dent. 1972; 28:379.
20. Urstein M, Fitzig S, Moskona D. Cardash HS. A clinical evaluation of materials used in registering interjaw relationships. J. Prosthet Dent. 1991; 65(3):372-7.
21. Walls AW, Wassel RW, Steele JG. A comparison of two methods for locating the intercuspal position whilst mounting cast on an articulator. Journal of Oral Rehabilitation. 1991; 18(1):43-8.
22. Wirth CG, Aplin AW. An improved interocclusal record of centric relation J. Prosthet Dent. 1971; 25:2 79.
23. Woelfel JB. New device for accurately recording centric relation. J. Prosthet Dent. 1986; 56(6):71 6-27.
|